September 18, 2016
Ontario’s health care system, and particularly our home and community care services, is undergoing significant change. Both provincial and federal governments have started processes which will restructure and redefine home and community services that are supposed to support and keep ageing Ontarians in their own homes for as long as possible. There is (unfounded) widespread fear that Canada’s ageing Baby Boomers will bankrupt our Medicare system.
The impetus for change in Ontario include: the Auditor General’s Report, which severely criticized the efficiency of community care access centres (CCACs), which encouraged Health Minister Eric Hoskins to launch a restructuring of home and community care services; the need to contain or manage the growth of health costs; and, finally, collective bargaining underway with the Ontario Medical Association regarding future service fees and funding for physician services.
In Ontario, the change vision is called Patients First and is being slowly rolled out: Pilot projects around “Bundled Care” are in place; “Primary Care” is a Ministry priority; CCACs are being phased out and the LHINs are mandated to implement the 10 steps in a provincial home and community care Roadmap.
Finance ministers are debating health care costs and how these will be shared across provincial and federal jurisdictions. Their focus is on implementing efficiencies and increasing transfers to provinces to cover the projected funding gap. However, remarkably little attention is being paid to changing the model of health care and ways of financing it. At both the national and provincial levels, a key determinant of what home and community care services Ontarians can expect to get in the future will be determined by how services are funded and how much funding is invested and earmarked for such services.
Care Watch believes strongly that the time has come to have serious discussions about how we will fund home and community care, to arrive at a consensus and begin to take action to ensure that our elected officials are aware of our preferences and expectations.
Many scholars, journalists, politicians and advocacy groups have looked at health care statistics and argued for ways of addressing the funding gap (for a recent review see HealthPapers 2016). Care Watch enters this funding debate with two premises: An equitable home and community care policy must (1) be based on the same principles as the Canada Health Act (CHA), and (2) be supported by a funding commitment that originates in the tax system.
The CHA, whatever its shortcomings, has several major strengths and one serious limitation. The major strengths are its principles of public administration, comprehensiveness, universality, portability and accessibility. The serious limitation is that the Act only covers medically necessary services received in hospitals or from physicians. It does not cover services that people receive in their homes. Thus, most of the services needed by an ageing population are not covered.
Critical voices recognize that hospitals were developed as sites for dealing with acute care, but chronic care is what an ageing population needs. Elderly patients are reasonably well served by acute care medicine, but chronic care alternatives are scarce. Needed community supports – to keep people out of expensive hospitals as they age – are even scarcer.
There is broad consensus that access to home and community care services should be based solely on a needs assessment, and Care Watch agrees. However, there has been no real discussion about how to pay for such services to ensure equity, and that access is based on needs rather than economic ability.
So, how can we ensure equitable access to home and community care services?
An ageing population requires home and community care legislation that is built on the same principles as the CHA. To do this will take a major infusion of funds. Initiatives such as bundled care or integration of services, basically efficiency measures, cannot begin to generate such funds. We need to identify funding approaches that can place home and community care on the same solid foundation as services now covered by the CHA. The debate will be acrimonious (challenging the status quo means threatening existing privilege), but must occur or senior citizens, when they most need the security of services, will be disenfranchised.
In 2010, Care Watch issued a pamphlet titled A Pragmatic Proposal which emphasized the importance of securing sustainable funding for building a home and community care model that can address the needs of Ontario’s ageing population. At that time, such services kept slipping off the policy table as “crises” in acute care grabbed the headlines. Having watched this happen time and again, we were convinced that home care dollars would continue to be leached by acute care priorities. The only way to stem this leaching would be a funding mechanism that quarantined home care funds from acute care use, in other words, designated funding. Our basic position has not changed in the ensuing years. What may have changed is a political willingness to recognize that the status quo is not an option.
Care Watch is convinced that designated funding options need to be discussed now so that elderly persons and their families are not bearing all of the costs.
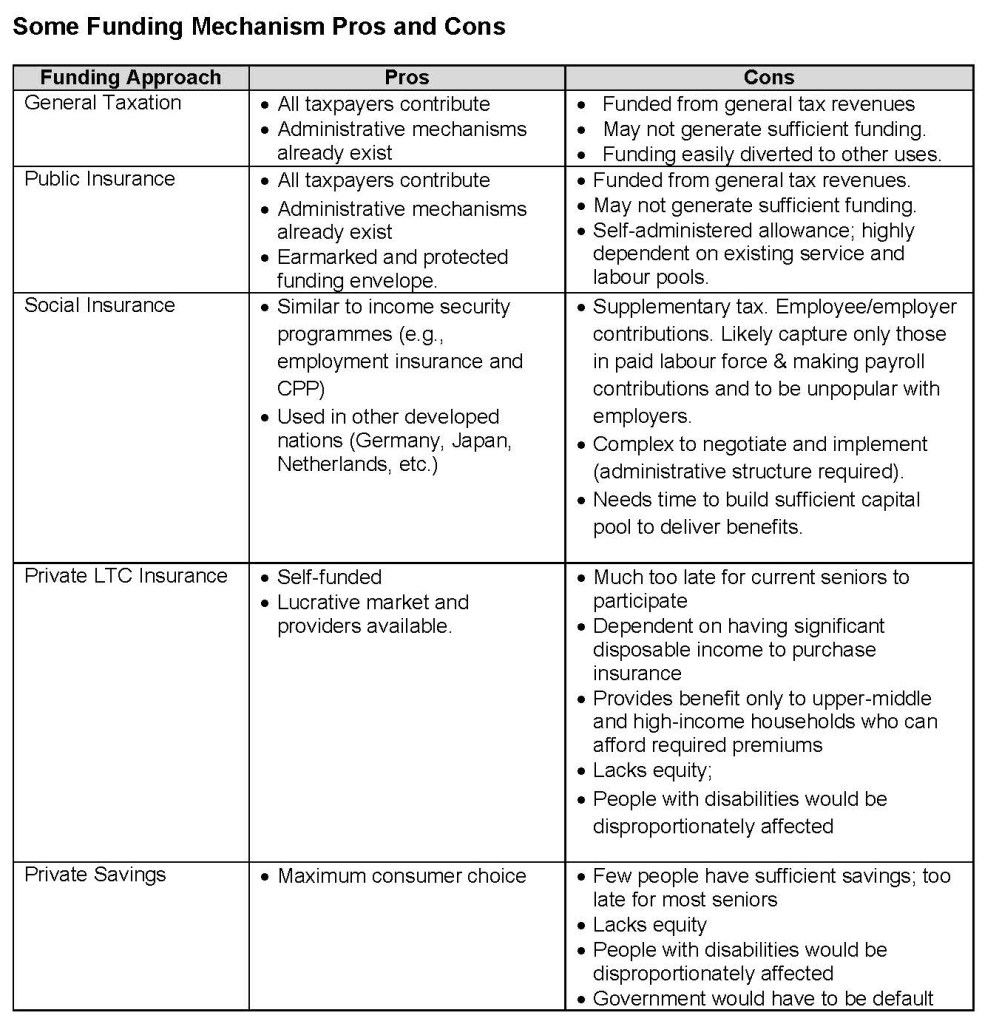
But how can we generate the necessary funds to pay for services? Several funding mechanisms are possible – all with pros and cons:
- General Taxation (Torjman 2016) – Funding through general tax revenues;
- Public Insurance [1] (Hebert 2016) – Funding through general tax revenues with a dedicated separate budget program to protect the funds;
- Social Insurance (Grigon 2016) –Funded through a supplementary tax (e.g., a payroll tax like the CPP or OHIP supplement).
Other options exist – such as diverting funds from medical services to invest in LTC (Emery 2016); developing private LTC insurance schemes; providing incentives for inducing people to save; and developing the informal care market through carers allowances (Blomquist & Bushy 2016). These exist in various jurisdictions, but none meet the service principles – i.e., public administration, comprehensiveness, universality, portability and accessibility – underlying the CHA. Thus Care Watch does not support them.
The ageing of Ontario’s population has been obvious at least since 2011. A serious conversation about funding a home and community care policy that parallels that of the Canada Health Act is overdue. The tax system is the only source for generating the guaranteed funding that is necessary. The time for action is now.
Footnote:
[1] This Quebec legislative proposal also provided for an allowance managed by individuals and their families to purchase services from community organizations (e.g., meals on wheels), social economy agencies (care, transportation, etc.), and private organizations or to hire personal caregivers. An election intervened before the program was implemented.
References:
Blomquist, Ake and Colin Bushy. (2016). Determining the public/private mix: Options for financing targeted universality in long-term care. HealthPapers 15 (4), 25-30.
Chappell, Neena L. (2011). Population Aging and the Evolving Care Needs of Older Canadians: An overview of the policy challenges. IRPP Study. No. 21. October 2011
Deber, Raisa B. and Audrey Laporte (2016). Funding long-term care in Canada: Who is responsible for what? HealthPapers 15 (4), 36-40.
Emery, J. C. Herbert. (2016). A fifth option for funding long-term care in Canada – shift the resources from medical treatment and universal pension entitlements. HealthPapers 15 (4), 41-44.
Frank, Stephen (2016). Recognizing the magnitude of the challenge. HealthPapers 15 (4), 51-54.
Grignon, Michel (2016). Funding for long-term care: Why public Insurance makes sense. HealthPapers 15 (4), 21-24
Hebert, Rejean. (2016). Still-born Autonomy Insurance plan in Quebec: An example of a public long-term care insurance system in Canada. HealthPapers 15 (4), 45-50.
Ontario. (2015). Patients First: A Roadmap to Strengthen Home and Community Care. Ministry of Health and Long Term Care.
Owens, Adams and Sharon Vanin (2016). Funding long-term care in Canada: Issues and Options. . HealthPapers 15 (4), 7-20.
Torjman, Sherri. (2016). Long term commitment for long-term care. HealthPapers 15 (4), 31-35.
Williams, A. Paul, Janet Lum, Frances Morton-Chang, Kerry Kuluski, Allie Peckham, Natalie Warrick, Alvin Ying (2016). Integrating Long-Term Care into a Community-Based Continuum Shifting from “Beds” to “Places”. IRPP Study. No. 59. February 2016.
